Model III – Deeper Brain Structure Dysfunction
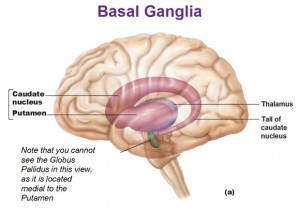
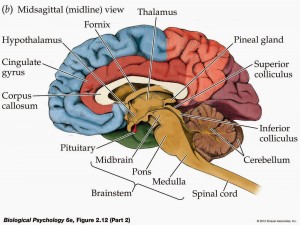 Another explanation for ADHD is a problem with the basal ganglia, and the corpus callosum just above the basal ganglia (Biederman et al, 2004). These are deeper brain structures, which serve as “switching stations” for information. In a typical brain, information passes through these structures, and a decision is made. If the information is important, then it is re-routed to the appropriate areas of the brain for processing; if it is not important, it is ignored and not passed on for additional processing. In an ADHD brain, however, relevant information sometimes is not passed on, and irrelevant information sometimes is not ignored. This means, in effect, that other areas of the brain must sometimes work without the information they need (which would lead to making premature decisions and acting on them quickly, or impulsivity), and must sometimes work with too much information (which would lead to poor decisions sometimes and distractibility other times).
Another explanation for ADHD is a problem with the basal ganglia, and the corpus callosum just above the basal ganglia (Biederman et al, 2004). These are deeper brain structures, which serve as “switching stations” for information. In a typical brain, information passes through these structures, and a decision is made. If the information is important, then it is re-routed to the appropriate areas of the brain for processing; if it is not important, it is ignored and not passed on for additional processing. In an ADHD brain, however, relevant information sometimes is not passed on, and irrelevant information sometimes is not ignored. This means, in effect, that other areas of the brain must sometimes work without the information they need (which would lead to making premature decisions and acting on them quickly, or impulsivity), and must sometimes work with too much information (which would lead to poor decisions sometimes and distractibility other times).
This explanation is a good one, and is supported by research:
- For example, studies have shown that children with ADHD show different levels of activity of the frontal-striatal cerebellar circuits, or the neurons connecting the front of the basal ganglia to the pre-frontal lobes (Vaughan et al, 2012). This would explain some of the executive function difficulties noted earlier, particularly difficulties in working memory and paying attention.
- Studies have also shown that people with ADHD have less activity in the ventral striatum (which relies heavily on D1 and D2 dopamine receptors), or the circuits on the underside of the basil ganglia that connect it to the limbic or reward system (Shaw et al., 2014). This could explain why people with ADHD may become bored easily, seek novelty, and prefer immediate rewards rather than long-term ones.
- Studies have also shown people with ADHD have disruptions in the links and activity between the basil ganglia and sensorimotor cortex (Shaw et al., 2014). This could explain why people with ADHD have difficulty inhibiting motor responses; in other words, this would explain why they act impulsively.
- Vetrivelan et al., (2010) report that the basal ganglia is involved in sleep regulation, specifically the dopamine neurons. This is consistent with other studies which show that almost 90% of people with Parkinson’s disease (which involves degeneration of the neuron circuits in the basal ganglia) suffer from sleep disturbances. Kirov et al., (2012) notes that many studies have shown that ADHD children have sleep disturbances. They studied ADHD and non-ADHD children in their sleep lab and found that children with ADHD tended to spend more time in dreaming or REM sleep. This held true both for those who had and had not been given stimulants (none of the children were taking stimulants at the time of the study). Further, children with greater attention problems spent the most time in REM sleep.
- (Shaw et al., 2014) performed MRIs on 270 children and teens with ADHD (82% showed both attention problems and hyperactivity), as well as another 270 without ADHD, and studied the growth of the overall surface and in the different areas of the basil ganglia. They scanned participant brains at various times between the ages of 4 and 19.
- They found at the start of the study that the basil ganglia was smaller in children with ADHD.
- Participants with and without ADHD showed similar patterns of growth in the surface area of the basil ganglia, as well as in the different structures of the basil ganglia. However, for ADHD children, some structures of the basil ganglia, and so failed to “keep up.” In other words, some structures grew at such a slower rate that they became relatively smaller over time.
- They saw trend most often in the structures that linked the basil ganglia to the limbic or reward system (the ventral striatum) and to the prefrontal cortex. This supports the finding that people with ADHD prefer immediate rewards, and show difficulty with attention and planning, as noted above.
- These differences persisted from childhood into adolescence. Thus, a comparatively smaller basil ganglia was seen at the start of the study, and comparatively smaller structures of the basil ganglia were still seen at the end of the study.
- When they compared starting size and growth over time of the basil ganglia for children with ADHD who did and did not take stimulants, they found no differences. Thus, stimulant medication did not appear to have any effect on the size or growth of the basil ganglia or its structures.
- Further, this model also allows us to explain why stimulants like Ritalin would be helpful. In short, Ritalin improves the functioning of the transport molecules in the basal ganglia. These molecules carry dopamine from one neuron to a second neuron, wait while the neurotransmitter’s “message” from the first neuron is “heard” by the second one, and then carry the dopamine back to the first neuron. Focalin (a specific shape of the Ritalin molecule) has been shown to affect the basal ganglia more than other brain structures, which would further explain the impact of stimulants like Ritalin.
- If it helps, think of a friend who sends you a text message asking if you want to grab a bite to eat, then waits for your reply. Dopamine is like the text message with your friend’s question, and the transport molecules are the app on your phone which accepts the text from your friend and stores it on your phone for you to read.
- Imagine that sometimes your phone plays a sound when messages arrive… but often it does not. It will be hard for you to know your friend asked you a question, and hard for your friend to know whether you got their text. Ritalin is sort of like an improvement to the messaging app; for a time, it will make sure a sound is always played when a text message arrives, and repeated a moment later in case you missed it.
Thus, this model is more specific than the frontal lobe dysfunctional model, and easily explains why a problem in the deeper brain would cause problems in the functioning of the frontal lobes. Further, studies have supported the role of the basal ganglia in ADHD, as well as supported that other areas of brain functioning (sleep regulation, impulse control, attention, working memory…) are linked to areas of the brain that connect directly to the basal ganglia.
Unfortunately, this model is not perfect either:
- About 30% of individuals with ADHD do not respond to stimulants like Ritalin (Biederman et al, 2004), though they may respond to other drugs, such as MAOIs, tricyclic antidepressants, or SSRIs. The problem is that this model does not explain why stimulants would not work, and why these others drugs would.
- As with the Pre-Frontal and Frontal lobe model, the model doesn’t explain why two individuals with ADHD will show some, but not all, of the same problems.
- It is possible that there is more than one cause for ADHD, however, and so perhaps we need more than one model.
While not perfect, this seems the best model we have for how ADHD works. Next post… Is There A Genetic Cause For ADHD?